Pressure in the ear, humming, ringing, or not difficulty hearing, but rather “difficulty understanding what is heard”… But have you ever considered that these complaints might originate not from the ear, but from the jaw joint?
Modern approaches in anatomy, neurology, and manual therapy point to the existence of a “silent bridge” between the ear and the jaw: the auriculotemporal nerve. In this article, we will explore the anatomical, neurological, and embryological roots of the connection between the temporomandibular joint (TMJ) and hearing. We will also present scientific data supporting the relaxing effects of the Atlas Therapy approach on sensory nerves and how it contributes to auditory comprehension.
Anatomical and Functional Features of the Auriculotemporal Nerve
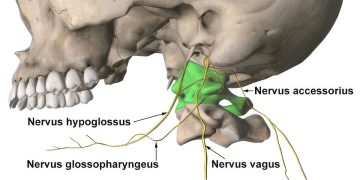
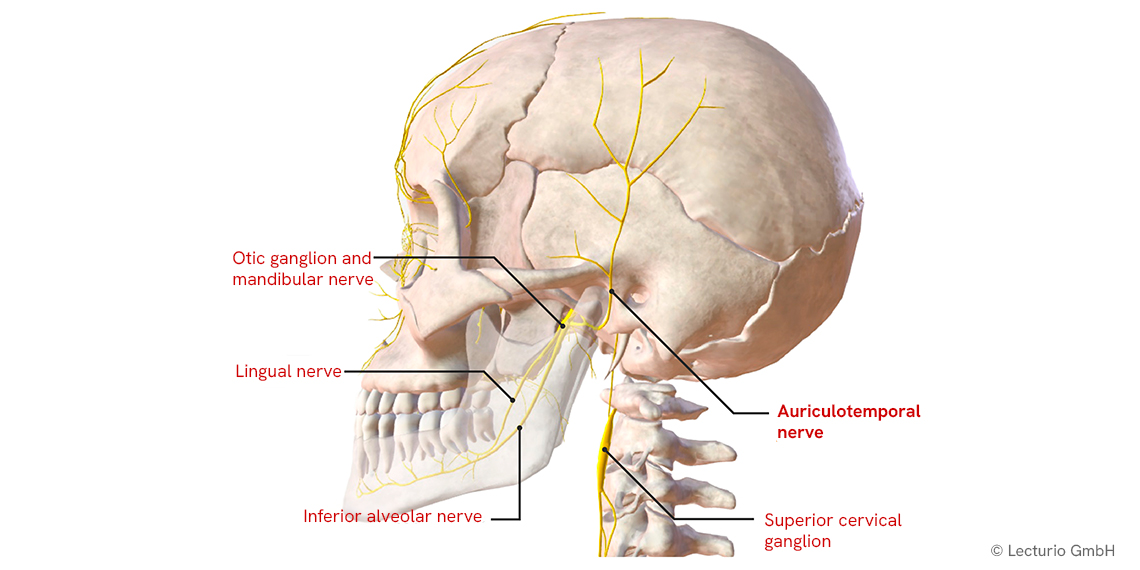
The auriculotemporal nerve branches from the mandibular nerve, which is the third division of the trigeminal nerve (CN V). It passes posteriorly from the temporomandibular joint (TMJ), travels in front of the ear, and extends toward the temporal region.
The main functions of this nerve include:
-
Providing sensory innervation to the TMJ capsule,
-
Sending sensory branches to the auricle, external auditory canal, and the outer surface of the tympanic membrane,
-
Innervating the skin of the temple,
-
Connecting via parasympathetic fibers to the parotid gland (salivary gland in front of the ear).
Due to its close path to the TMJ, any structural imbalance or dysfunction in the jaw joint may cause mechanical pressure, tension, or reflex responses on the auriculotemporal nerve—resulting in symptoms perceived in both the jaw and the ear.
The Jaw-Ear Connection: Anatomical, Neural, and Embryological Foundations
1. Shared Neural Networks (Neuroanatomical Connection):
The jaw joint is directly connected to the ear through the mandibular branch of the trigeminal system. The auriculotemporal nerve provides sensory input to both the TMJ and the external auditory canal. As a result, a pathology in the jaw region may be perceived in the ear. In fact, cerebral projections of the trigeminal system can cause pain and sensory inputs to be misinterpreted in different locations—a phenomenon known as referred pain.
2. Anatomical Proximity:
The TMJ is located anterior to the temporal bone, with the middle ear cavity on the other side. A very thin bony wall separates the two. Additionally, the petrotympanic fissure in this region provides a mechanical connection between the TMJ and the middle ear. Posterior displacement of the mandibular condyle may influence middle ear pressure via these structures.
3. Embryological Commonality:
The TMJ and middle ear structures develop embryologically from the same origin—the Meckel’s cartilage. This may leave residual connective tissues between the jaw joint and the ear. Notably, the discomalleolar ligament creates a direct connection between the TMJ and the “malleus” bone in the middle ear. TMJ dysfunction may affect the middle ear through this ligament.
4. Muscle–Eustachian Tube Relationship:
Masticatory muscles such as tensor veli palatini and tensor tympani are functionally linked to the Eustachian tube and auditory ossicles. Increased tone or spasm in these jaw muscles can impair Eustachian tube function, leading to a feeling of ear pressure and auditory blurring.
Scientific Findings: The Link Between TMD and Auditory Perception
Temporomandibular joint disorder (TMD) can affect not only jaw and head pain but also the auditory system. Some notable studies on this subject include:
-
Kitsoulis et al. (2011): In a study involving 464 participants, those with moderate to severe TMJ dysfunction showed reduced speech frequencies and hearing loss. While those with mild TMD had normal hearing, low-frequency hearing loss was more prominent in severe cases.
-
Naderi et al. (2023): In individuals presenting with otological symptoms (ringing, fullness, humming) but normal ENT examinations, TMJ dysfunctions were identified. Following manual and conservative treatments, up to 70% improvement in ear symptoms was reported.
-
Kijak et al. (2020): Anatomical variations in the petrotympanic fissure were shown to affect the relationship between TMJ and tinnitus. In individuals with narrowing or rotational issues in this fissure, improvement in jaw function was accompanied by a reduction in tinnitus.
These findings demonstrate that balancing the jaw joint may influence not only pain but also the quality of hearing and auditory comprehension.
Temporomandibular Joint Manipulation with the Atlas Therapy Approach
Atlas Therapy is a manual therapy approach that aims to balance the uppermost cervical vertebra—the atlas (C1)—along with the entire body’s biomechanics and neural communication.
Atlas Therapy applications to the TMJ aim to:
-
Guide the mandibular condyle into a physiologically appropriate position,
-
Reduce joint capsule tension,
-
Alleviate hypertonicity or spasm in masticatory muscles,
-
Regulate pressure and neurogenic stimulation on the auriculotemporal nerve.
During these manipulations:
-
A “click” sound may be heard—an indication of gas release within the joint,
-
Subsequently, the person may feel lighter jaw movements, ear clarity, and a sense of relaxation in the head-neck region.
Such examples show that unexplained sensory symptoms around the ear may originate from dysfunctions in the jaw and neck alignment.
Many ear-related complaints may not stem from the ear itself, but rather from other sources in the nervous system. The auriculotemporal nerve serves as a sensory bridge between the jaw and the ear. Tension or irritation in this nerve may not affect hearing itself, but rather the comprehension of what is heard.
Atlas Therapy targets the regulation of neural communication via the jaw joint and cervical segments. This can contribute to the alleviation not only of jaw or neck pain, but also of symptoms such as ear fullness, humming, or auditory blurring.
If there is a “perceptual confusion” in the ear, perhaps the solution lies not within the ear—but in the alignment of the jaw and neck.
References:
-
Kijak E. et al. Anatomical Features of Petrotympanic Fissure and Tinnitus in TMD, Pain Res Manag, 2020.
-
Kitsoulis P. et al. TMD and Hearing Loss, BMC ENT Disord, 2011.
-
Naderi Y. et al. Otologic Symptoms and TME Dysfunction, BMC Oral Health, 2023.
-
Olson H. et al. Auriculotemporal Neuralgia and Manual Care, J Contemp Chiropr, 2021.
-
Netter, F. Atlas of Human Anatomy, Elsevier, 2018.